-
Tip:
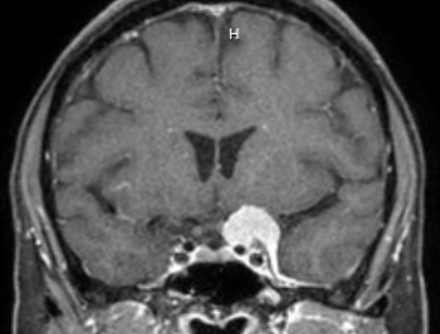
non-contrast CT may miss the tumor because the tumor has the same radiodensity as adjacent brain parenchyma
-
Untreated tumors may grow slowly, but growth often stops after menopause
-
Endonasal or transcranial surgery is advised if
-
Vision attributable to tumor is declining
-
Mass is large or enlarging
-
Surgical risk is acceptable
-
Expect skilled surgery to improve or stabilize vision in 75%, worsen vision in less than 25%
-
Trap:
large and invasive lesions pose extra surgical hazards and often cannot be entirely excised without harming vision
-
Trap:
if the tumor has invaded the optic canal, a feature not easily evident on imaging, the prognosis for post-operative visual recovery is less favorable
-
Radiation therapy is preferred over surgery to stabilize vision if the surgical risk is high or surgery leaves a large residual or recurring tumor
-
Trap:
radiation therapy does not improve vision, may rarely worsen it after months to years, and may pose long-term risks of stroke, hypopituitarism, dementia, vasculopathy, and development of a second intracranial tumor