Pituitary Adenoma
- Tumor caused by neoplasia of the anterior pituitary gland
- Young and middle-aged women are most affected
- Visual loss is usually slow, but may be acute from tumor hemorrhage (“pituitary apoplexy”)
- Most tumors that affect vision are endocrinologically silent
- Brain MRI is often diagnostic, but…
-
Trap: other masses can mimic pituitary adenoma on MRI
- Transsphenoidal surgery usually provides dramatic visual improvement, but…
- Large extrasellar extension may pose extra surgical risk
- Marked pre-operative vision impairment adversely affects visual outcome
-
Core clinical features
- Subacute or chronic visual loss, often monocular
- Sudden visual loss usually means tumor hemorrhage in “pituitary apoplexy”
- Nerve fiber bundle and/or hemianopic defect
- Afferent pupil defect
- Optic discs appear normal or pale
-
Possible accompanying clinical features
- Chronic or new headache
-
Hormonally-silent tumors are typically larger and more vision-impairing at presentation than the following hormonally-active tumors
- Prolactin-secreting: galactorrhea, amenorrhea, decreased libido, impotence
- Growth hormone-secreting: acromegaly, gigantism
- Corticotrophin-secreting: cushingoid features, diabetes, myopathy
- Thyrotropin-secreting: hyperthyroidism, goiter
- Gonadotropin-secreting: precocious puberty, decreased libido
-
Imaging features
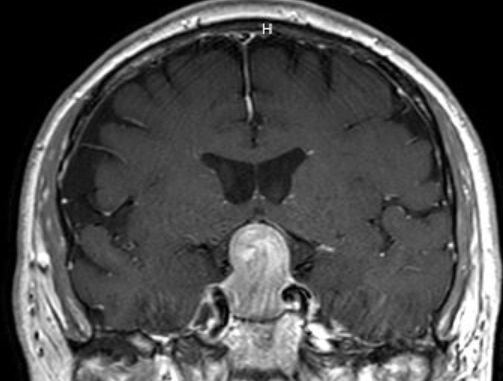
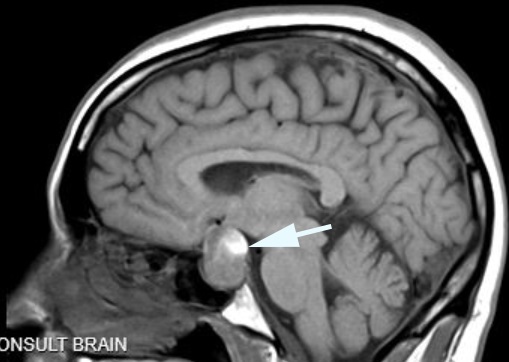
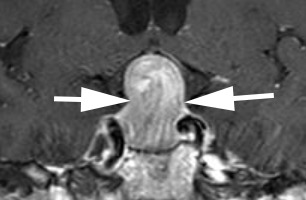
- Avidly and heterogeneously enhancing mass originating in the pituitary gland with extension into the suprasellar space
- Belt-like constriction between the sellar and suprasellar components of the tumor because of a tight diaphragma sellae
- Meningioma
- Craniopharyngioma
- Rathke cleft cyst
- Pilocytic astrocytoma (Optic glioma)
- Carotid aneurysm
- Germinoma
- Pituitary hyperplasia
- Sinonasal cancer
- Metastatic cancer
- Arachnoid cyst
- Epidermoid and dermoid cysts
- Histiocytosis
- Sphenoid sinusitis or mucocele
- Lymphocytic hypophysitis
- Pituitary abscess
- Sarcoidosis
- Order brain MRI
-
Trap: watch out for the following masses that mimic pituitary adenoma on MRI: pituitary hyperplasia, craniopharyngioma, metastasis, germ cell tumor, aneurysm, lymphocytic hypophysitis
- Order serum prolactin: >200ng/ml signals a prolactinoma, which is usually treated first with a dopamine agonist (cabergoline)
-
Tip: non-prolactinoma sellar masses often elevate prolactin (“stalk effect”), but never above 200ng/ml
- Refer non-prolactinomas to a neurosurgeon
- Prolactinomas often shrink rapidly with dramatic visual improvement following dopamine agonist (cabergoline) therapy, making surgery unnecessary, but…
-
Trap: dopamine agonist therapy is not always effective or tolerated and must be maintained indefinitely
- Non-prolactinomas are effectively managed by transsphenoidal or wide endonasal surgery with visual improvement or stabilization in >90%
- If the tumor must be approached transcranially, visual improvement is less likely and visual damage is more likely
-
Tip: pituitary apoplexy must be managed with prompt hormonal replacement and fluids, but surgery can probably be briefly delayed without adverse consequences to allow for metabolic stabilization
- Regrowth of tumor is uncommon but may occur many years after initial treatment, so you must maintain imaging and clinical surveillance
- Radiation therapy is reserved for non-candidates for surgery, large post-operative residual tumors, or tumor regrowth