Pilocytic Astrocytoma (Optic Glioma)

- Congenital low-grade (WHO Grade 1) astrocytoma of the optic nerves, optic chiasm, and hypothalamus (“optic glioma”)
- Usually discovered before age 20 years
- Neurofibromatosis type 1 is present in 30–50%
- Present in 15% of patients with neurofibromatosis type 1
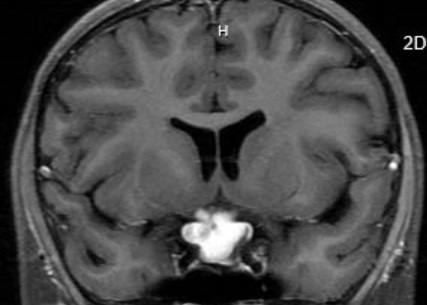
- MRI shows an intrinsic mass in the optic nerve, optic chiasm, and/or hypothalamus
- No biopsy is necessary if imaging is distinctive
- Chemotherapy is often used but its benefit is uncertain as controlled trials have not been performed
- Surgical resection of the optic nerve is reserved for unsightly proptosis when the affected eye has no light perception
-
Core clinical features
- Stationary or progressive visual loss in one eye or both
- Reduced visual acuity and visual field defects in one or both eyes
- Afferent pupil defect
- Optic discs appear normal or pale (or elevated if an orbital tumor involves the distal optic nerve)
- Possible accompanying clinical features
-
Imaging features
- Brain/orbit MRI shows enlargement or signal alteration within the optic nerve, optic chiasm, and/or hypothalamus
-
Tip: pilocytic astrocytoma is unusual among optic nerve lesions in causing marked enlargement of the nerve and/or chiasm together with avid enhancement
- Other orbital and sellar region tumors
- Optic neuritis
- Neuromyelitis optica
- Lymphocytic hypophysitis
- Sarcoidosis
- Metastatic cancer
- Hematopoietic cancers, including lymphoma
- Langerhans cell histiocytosis
- Order orbit-based MRI, which is usually diagnostic
- Biopsy the lesion only if the imaging features are not classic or a large exophytic component is present
- Tumor size and visual function often remain stable in untreated patients
- Visual decline may be caused either by tumor growth, tumor production of extracellular matrix, or reactive meningeal hyperplasia
- Intraorbital tumors may have an intracranial component, but they do not spread intracranially
-
Trap: do not treat a tumor apparently confined to the orbit, except when there is disfiguring proptosis and a blind eye, in which case excision of the intraorbital optic nerve, sparing the eye and extraocular muscles, may be indicated
- Place a ventriculoperitoneal shunt for obstructive hydrocephalus
- Consider chemotherapy for patients under age 9 whose tumors are growing, involving the optic chiasm or hypothalamus, causing severe vision loss, worsening vision, or hypothalamic dysfunction
-
Trap: there are no large controlled trials to affirm that chemotherapy is effective in this condition, but newer agents, including MEK inhibitors, are showing promise
- Consider radiation therapy as an alternative to chemotherapy for patients older than 9 years
-
Trap: radiation therapy in patients with NF 1 carries a high risk of later occlusive vasculopathy and secondary tumors
- These tumors may rarely cause severe neuroendocrine morbidity or death