Occipito-Temporal Lesions
- Focal damage to posterior inferior temporal lobe causing poor visual recognition (“visual agnosia”)
- Common causes of unilateral lesions: stroke
- Common causes of bilateral lesions: Alzheimer disease, encephalitis, posterior reversible encephalopathy syndrome (PRES)
- Visual acuity is preserved with unilateral lesions
-
Tip: visual acuity testing may falsely suggest poor acuity if the patient has pure alexia
-
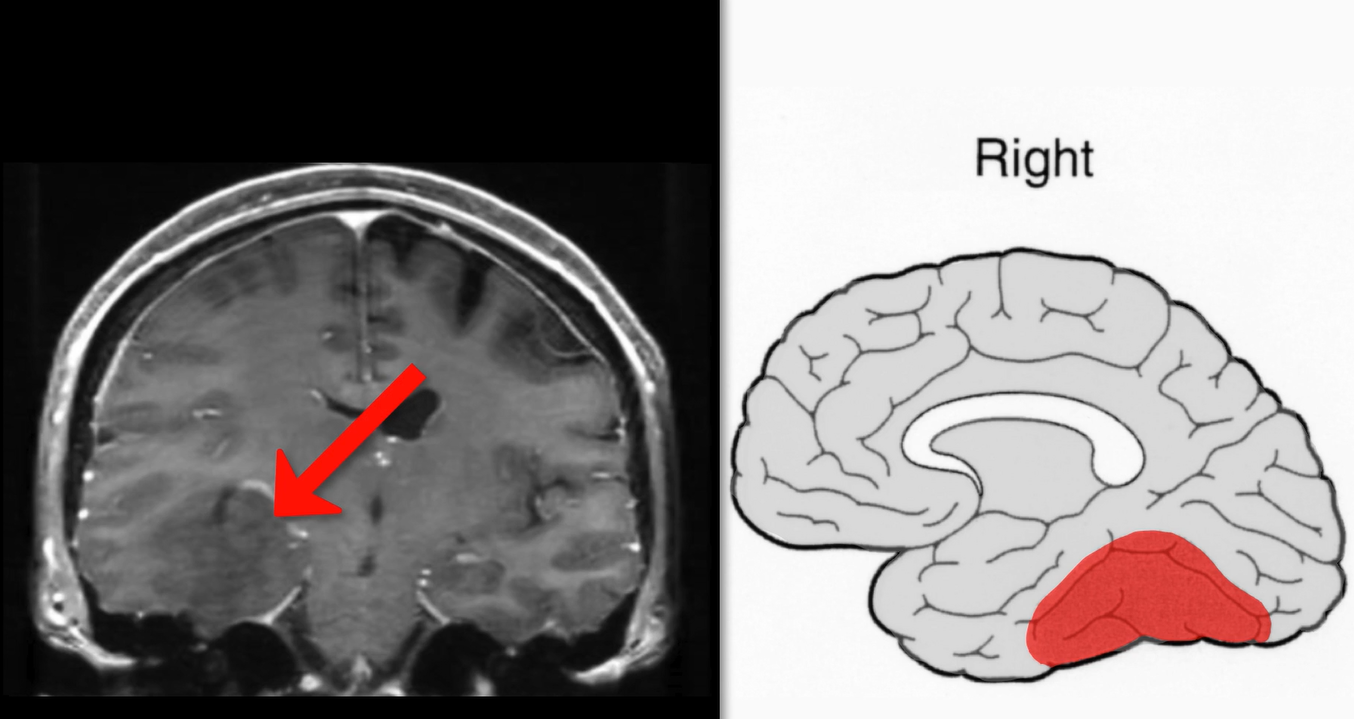
Right temporal lesion
- Homonymous hemianopia primarily affecting the left superior quadrants
- Topographical agnosia (difficulty following familiar routes)
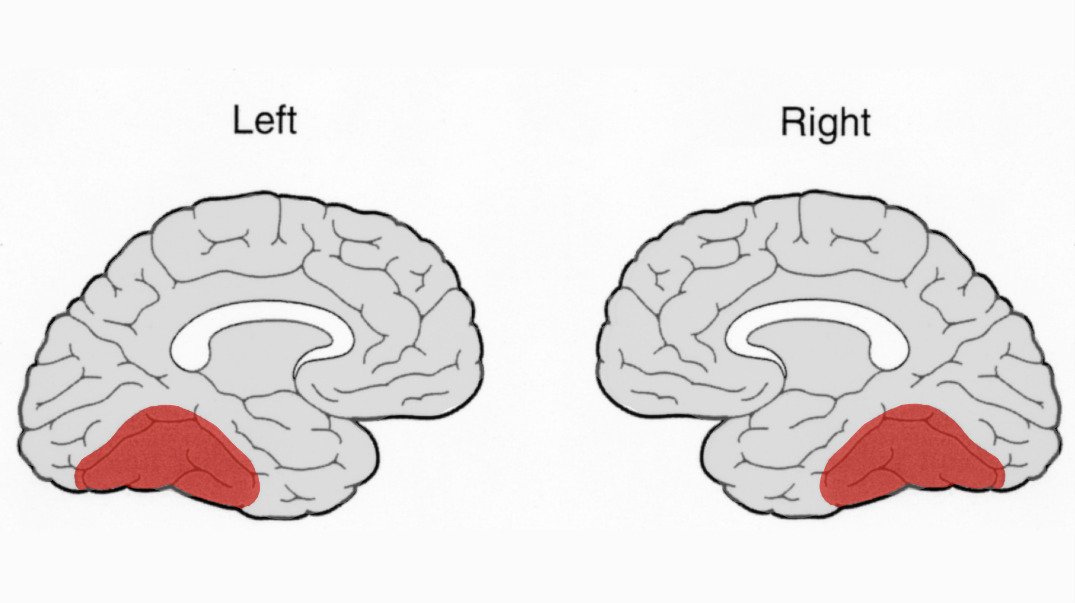
- Left temporal lesion
- Bilateral temporal lesions
- Reduced level of consciousness
- Developmental cognitive retardation
- Delirium
- Dementia
- Psychogenic unresponsiveness
- Poor cooperation
- Impaired communication
- Test visual acuity with tumbling Es or pictures in patients with alexia
- Test for prosopagnosia by displaying famous faces in magazines or by asking patients to identify companions
-
Test for visual object agnosia
-
Instruct patients to identify common objects
- If patients cannot identify common objects by sight, but can identify those objects by grasping them, diagnose visual object agnosia
- If patients cannot identify common objects by grasping them, but can describe how those objects are used, diagnose a naming disorder (“dysnomia”)
- If patients cannot describe how grasped objects are used, diagnose dementia or poor cooperation
-
Instruct patients to identify common objects
-
Test for alexia without agraphia
-
Instruct patients to read common words
- If patients cannot read common words, but can spell and write them to dictation, diagnose pure alexia (“alexia without agraphia”)
- If patients cannot spell or write common words, diagnose aphasia, poor cooperation, poor education, or cognitive impairment
-
Instruct patients to read common words
- Diagnosis of recognition deficits is often delayed because standard examinations do not assess them
- Patient responses are often falsely attributed to poor cooperation, depression, or dementia
- Alexia falsely suggests reduced vision
- Deficits may improve in stroke
- Deficits will worsen in dementia
-
Trap: widely-prescribed rehabilitative measures offer limited benefit