Unilateral Pontine Syndrome
- Core neuro-ophthalmic features
-
Possible accompanying neuro-ophthalmic features
- Lower motor neuron seventh nerve palsy
- Exotropia (“pontine exotropia”)
- Esotropia (from sixth nerve palsy)
- Skew deviation
- Gaze-evoked horizontal or upbeat nystagmus
- Saccadic pursuit
- Contralateral gaze deviation
-
Tip: various deficits may be seen in combination:
-
Unilateral gaze palsy + ipsilateral internuclear ophthalmoplegia (“1.5 syndrome”)
-
Unilateral gaze palsy + ipsilateral sixth palsy, creating esotropia in primary gaze position
-
Unilateral gaze palsy + ipsilateral internuclear ophthalmoplegia + ipsilateral lower motor facial palsy (“8.5 syndrome”)
-
Unilateral gaze palsy + ipsilateral internuclear ophthalmoplegia + skew deviation, creating hypotropia in primary gaze position
-
-
Possible accompanying neurologic features
- Ataxia
- Contralateral hemiparesis
-
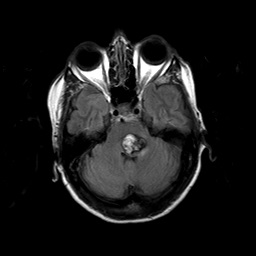

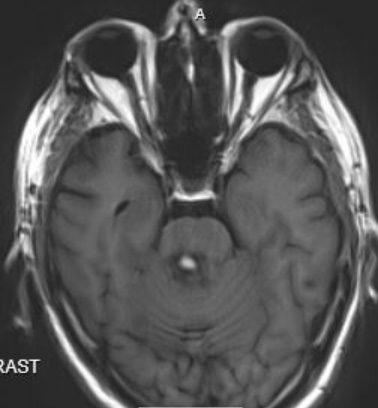
- MRI often shows the lesion
- Myasthenia gravis
- Fisher variant of Guillain-Barré syndrome
- Wernicke encephalopathy
- Frontoparietal stroke or hemorrhage
- Localize the lesion to the pons by noting that the Doll’s eye maneuver does not overcome a volitional gaze paresis
- Exclude myasthenia gravis, Fisher variant of Guillain-Barré syndrome, Wernicke encephalopathy, frontoparietal stroke/hemorrhage (frontoparietal stroke/hemorrhage causes contralateral neglect and contralateral hemiparesis)
- Order brain MRI
-
Trap: MRI may not reveal the lesion, especially in acute demyelination
- Depends on the cause
- Ocular motor manifestations may improve
- Other neurologic deficits tend to endure