( of )
Correct: 0
Incorrect: 0
A 50 year old woman is reporting slowly progressive vision loss in both eyes for the past year. The best-corrected visual acuities are 20/60 (6/18, 0.3) in each eye. There is no afferent pupil defect. Visual fields show bilateral centrocecal scotomas and the fundi look like this.
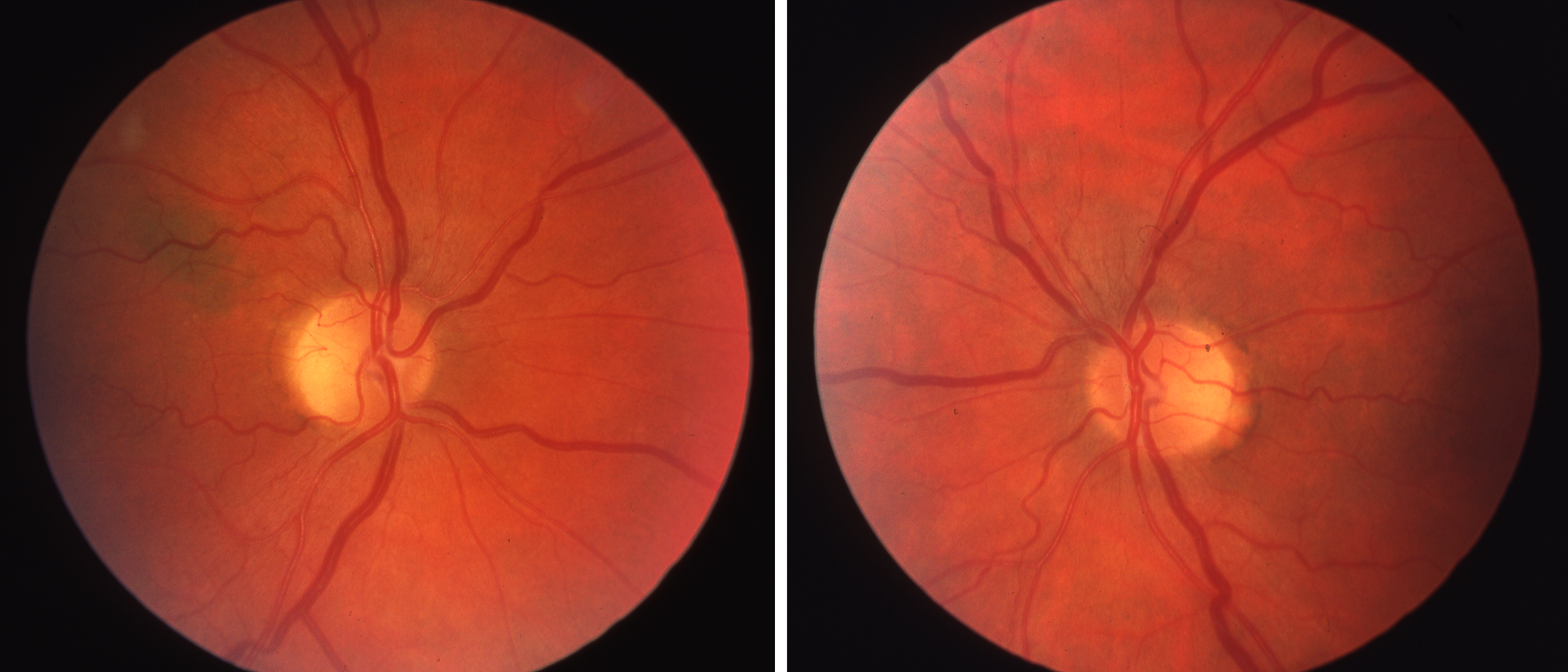
What might be causing the vision loss?
Incorrect
Incorrect
Correct!
The bilateral centrocecal scotomas on the visual field examination are the chief clues to localization and pathogenesis! Such defects occur from selective
damage to the retinal ganglion cells located in the fovea and between the fovea and optic disc. Their axons are unmyelinated. Toxic, nutritional, and
hereditary optic neuropathies do that kind of damage, affecting mitochondria.
Optic neuritis does not usually cause such centrocecal scotomas. It causes vision loss more quickly and preferentially affects myelinated axons, which lie mostly outside the maculopapillar bundles.
Compressive optic neuropathy would be expected to produce asymmetric damage to the optic nerves, and therefore an afferent pupil defect. It would not produce such centrocecal defects.
This patient had had been treated with ethambutol for tuberculosis. Optic nerve toxicity is rare at daily ethambutol doses below 15mg/kg unless the patient has reduced clearance from kidney disease. Scrupulous visual acuity and color vision monitoring is critical in patients treated with ethambutol because vision loss may become irreversible—and especially disabling as it is binocular!
Optic neuritis does not usually cause such centrocecal scotomas. It causes vision loss more quickly and preferentially affects myelinated axons, which lie mostly outside the maculopapillar bundles.
Compressive optic neuropathy would be expected to produce asymmetric damage to the optic nerves, and therefore an afferent pupil defect. It would not produce such centrocecal defects.
This patient had had been treated with ethambutol for tuberculosis. Optic nerve toxicity is rare at daily ethambutol doses below 15mg/kg unless the patient has reduced clearance from kidney disease. Scrupulous visual acuity and color vision monitoring is critical in patients treated with ethambutol because vision loss may become irreversible—and especially disabling as it is binocular!
Incorrect