( of )
Correct: 0
Incorrect: 0
This 50 year old woman awoke with blurred vision and imbalance. She had intractable hiccups, left-sided limb ataxia, numbness of the right hemibody and left face, and a comitant small right hypertropia.
Can you name the phenomenon you see in this video?
Incorrect
Incorrect
Incorrect
Correct!
 When the patient opens her eyes, the eyes shift back toward center. In other words, under closed lids, they have drifted conjugately to the
left. This phenomenon is called “ocular lateropulsion.” It reflects a marked tone imbalance within the central nervous system v
estibulo-ocular pathways, usually created by a lesion on one side of the medulla--here on the left. As a result, the eyes will be driven
conjugately to the lesioned (left) side when vision is interrupted by eye closure. Opening the eyes overcomes the driving force that results
from unbalanced vestibulo-ocular tone. Patients will often describe the sensation of being pulled toward one side (“pulsion”) and they may
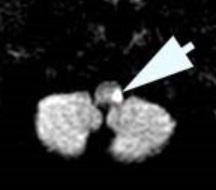
stagger to that side when walking, especially with eyes closed. The cause is often a dorsolateral infarction prompted by occlusion of the
posterior inferior cerebellar artery, which is, in turn, the result of a vertebral artery dissection.
When the patient opens her eyes, the eyes shift back toward center. In other words, under closed lids, they have drifted conjugately to the
left. This phenomenon is called “ocular lateropulsion.” It reflects a marked tone imbalance within the central nervous system v
estibulo-ocular pathways, usually created by a lesion on one side of the medulla--here on the left. As a result, the eyes will be driven
conjugately to the lesioned (left) side when vision is interrupted by eye closure. Opening the eyes overcomes the driving force that results
from unbalanced vestibulo-ocular tone. Patients will often describe the sensation of being pulled toward one side (“pulsion”) and they may
stagger to that side when walking, especially with eyes closed. The cause is often a dorsolateral infarction prompted by occlusion of the
posterior inferior cerebellar artery, which is, in turn, the result of a vertebral artery dissection.
Called a Wallenberg syndrome, this is the most common brainstem stroke in young and middle-aged adults. It always produces a constellation
of signs and symptoms, including ataxia, Horner syndrome, ipsilateral facial numbness, contralateral hemibody numbness, horizontal-rotary
jerk nystagmus, skew deviation, difficulty swallowing, and intractable hiccups (“singultus”). If the stroke causes a large hemispheric
cerebellar lesion, there is a concern for tonsillar herniation, which could be life-threatening. Hence the need for prompt diagnosis and
monitoring. Ocular lateropulsion is a quick diagnostic clue! By the way, there are other causes of horizontal gaze deviation, including an
acute cerebral hemispheric stroke, acute pontine stroke, focal cerebral seizures, and even acute peripheral vestibulopathy. They can be
distinguished by accompanying neurologic features.