( of )
Correct: 0
Incorrect: 0
This 60 year old man briefly lost consciousness. When he regained consciousness, this is how his eyes appeared.
Where is the offending lesion?
Incorrect
Incorrect
Correct!
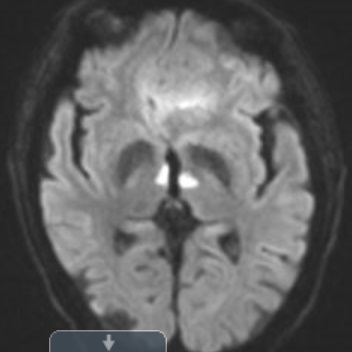 The lids are up and the eyes are down. Side gaze is reasonably intact. This combination of abnormalities--if acute--often localizes to the thalamus or the rostral dorsal
thalamic-midbrain junction. An expanding lesion here--usually a hemorrhage or an infarct
The lids are up and the eyes are down. Side gaze is reasonably intact. This combination of abnormalities--if acute--often localizes to the thalamus or the rostral dorsal
thalamic-midbrain junction. An expanding lesion here--usually a hemorrhage or an infarct
puts pressure on the posterior commissure, which lies immediately caudal to the thalamus. That commissure carries the pathway for upgaze. When it is damaged, the eyes cannot move up.
If the damage is severe, the eyes will deviate downward--the “sunset sign.” Less severe damage leaves the eyes in primary position, but they will not execute full upward gaze. Convergence
and retraction of the eyes may be visible with attempted upgaze. The mildest form of upgaze deficiency shows up as upbeat nystagmus. Lid retraction (“Collier’s sign”) is also common with
lesions in this region; its mechanism is unsettled. Another important cause of sunset eyes is sudden obstructive hydrocephalus from aqueductal stenosis or malfunction of a ventricular
shunt. Horizontal gaze, which is mediated by the pons, is left relatively intact, but you may have noticed that in this patient, it is interrupted by some aberrant convergence movements.
Incorrect