( of )
Correct: 0
Incorrect: 0
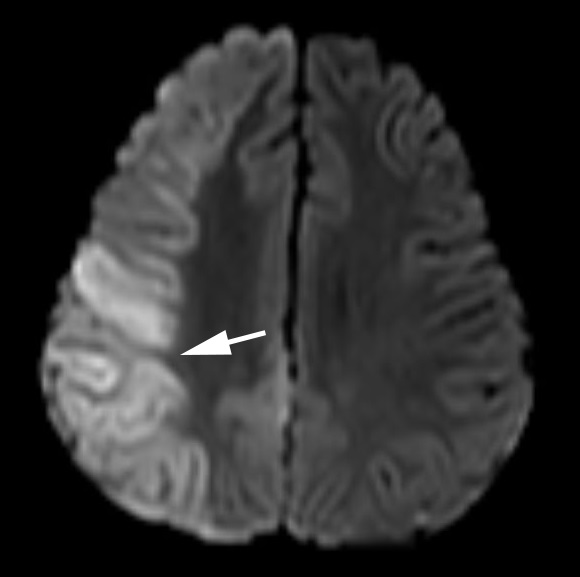
You are called to the bedside of this 68 year old woman, who recently had a stroke.
Where is the lesion?
Correct!
 The abnormality is a right gaze deviation. The patient cannot move her eyes to the left beyond the midline with saccades or pursuit. But with passive head movement
(the “oculocephalic” or “doll’s eye” maneuver), the eyes do move somewhat into left gaze. This dissociation between impaired volitional gaze (saccades, pursuit) and intact reflex gaze
(vestibulo-ocular reflex) is called a “supranuclear gaze palsy.” It signifies that the lesion lies in the cerebral hemispheres or diencephalon. The usual cause is a fresh hemorrhage or
infarct.
The abnormality is a right gaze deviation. The patient cannot move her eyes to the left beyond the midline with saccades or pursuit. But with passive head movement
(the “oculocephalic” or “doll’s eye” maneuver), the eyes do move somewhat into left gaze. This dissociation between impaired volitional gaze (saccades, pursuit) and intact reflex gaze
(vestibulo-ocular reflex) is called a “supranuclear gaze palsy.” It signifies that the lesion lies in the cerebral hemispheres or diencephalon. The usual cause is a fresh hemorrhage or
infarct.
In this setting, patients are occasionally able to execute contraversive saccades if they are implored by the examiner, in which case the gaze disorder is called a “gaze preference.”
The lesion will lie on the side of the gaze deviation (“the eyes point to the side of the hemispheric lesion”), usually in the parietal lobe. You can expect patients with this hemispheric
gaze disorder to display sensory and motor features of hemispatial neglect and sometimes contralateral hemiparesis or hemibody numbness. Focal seizures can cause contraversive horizontal
gaze deviation (“the eyes point away from the side of the lesion”), but the gaze deviation is episodic, and is often accompanied by contralateral head turn and tonic-clonic movements of
the face and extremities. Unilateral pontine lesions can cause contraversive horizontal gaze deviation (“the eyes point away from the side of the lesion”). Look for accompanying
ipsilateral limb ataxia and lower motor neuron facial palsy, contralateral extremity weakness and numbness, and nystagmus to help you localize the lesion to the pons.
Incorrect
Incorrect
Incorrect