Acute Cerebral Horizontal Gaze Deviation
- Sudden onset of sustained horizontal gaze deviation produced by a cerebral lesion
- Right gaze deviation is more common than left gaze deviation
- Right gaze deviation is associated with a right cerebral hemisphere lesion
- Left gaze deviation is associated with a left cerebral hemisphere lesion
- Common cause: fronto-parietal infarct or hemorrhage
- Uncommon cause: focal seizure
-
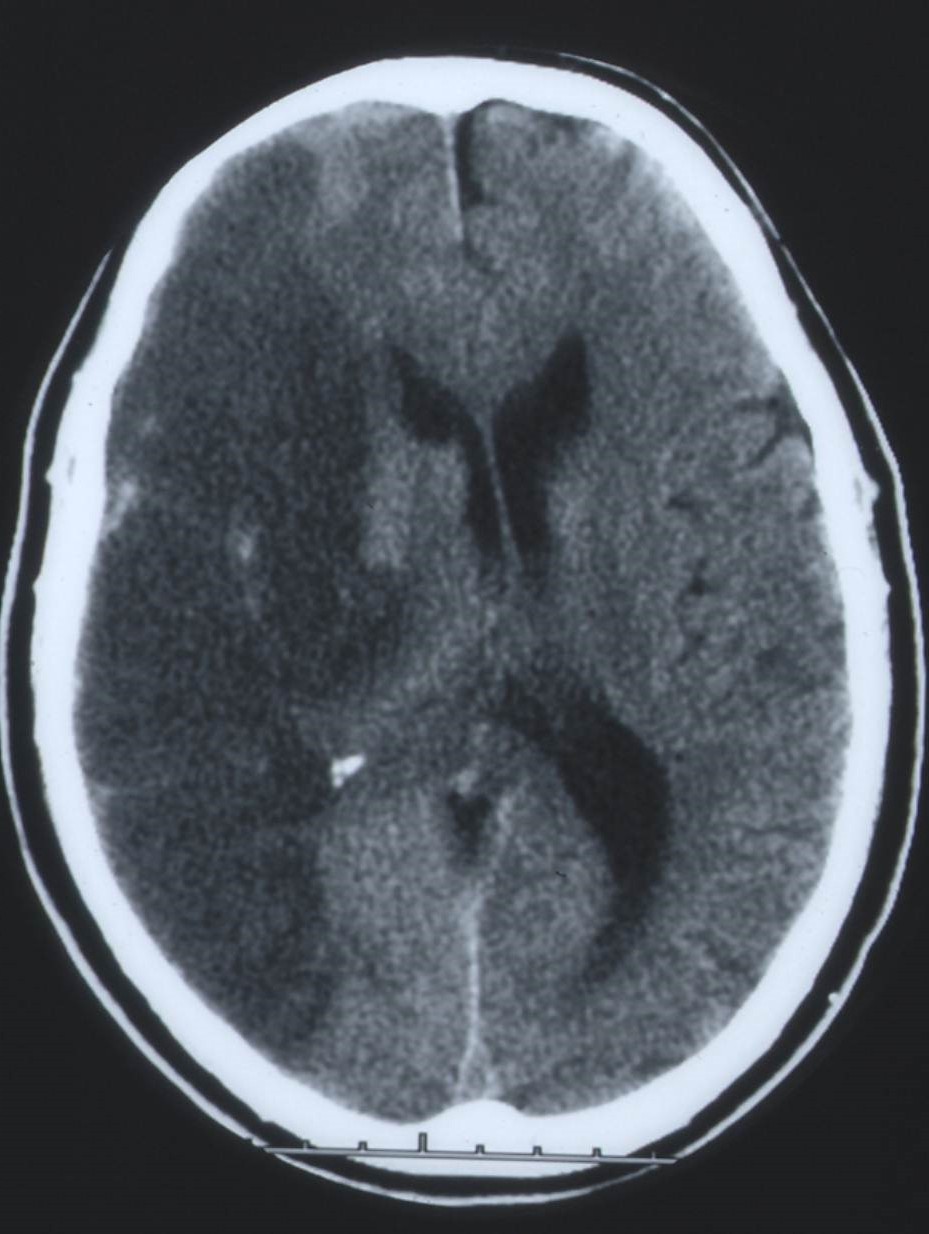
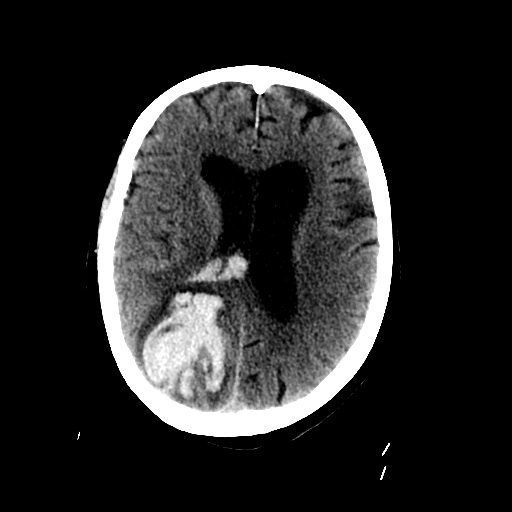
Cerebral hemispheric infarct/hemorrhage
- Eyes deviate conjugately to the side of the lesion (“horizontal gaze deviation”)
- Eyes may move to the midline or even to the opposite side with arousal and encouragement (“gaze preference”)
- Doll’s eye maneuver may bring eyes to the opposite side
- Vertical eye movements are usually intact but may be difficult to elicit
- Hemispatial neglect is present on the side opposite to the lesion
- Hemiparesis is present on the side opposite to the lesion
- Low arousal state
- MRI shows a cerebral hemispheric lesion on the side of the gaze deviation or preference
-
Focal seizure
- Eyes deviate conjugately to the side opposite to the seizure focus
- Jerk nystagmus with its fast phase to the side opposite to the seizure focus
- Head is often turned to the side opposite to the seizure focus
- Tonic-clonic movements of the limbs and face on the side opposite to the seizure focus
- In the post-ictal period, the eyes are often conjugately deviated to the side of the seizure focus and consciousness may be temporarily impaired
- Electroencephalography discloses hemispheric epileptic activity during a seizure and discloses hemispheric slowing post-ictally on the side of the seizure focus
- Pontine tegmental lesion on the side opposite to the gaze deviation and hemiparesis
-
Tip: in pontine gaze palsy, the vestibulo-ocular reflex fails to move the eyes across the midline to the opposite side
- Ocular lateropulsion: eyes deviate toward the side of a recent medullary lesion
-
Look for the following signs that help to distinguish these four entities
-
Cerebral infarct/hemorrhage
- Hemiparesis on the side opposite to the gaze deviation
- Doll’s eye maneuver and cold water caloric irrigation move the eyes to the opposite side
- Hemispatial neglect on the side opposite to the lesion
-
Cerebral focal seizure
- Head deviation to the side opposite to the seizure focus
- Tonic-clonic extremity movements on the side of the gaze deviation
- Eye deviation reverses direction post-ictally
-
Pontine tegmental dysfunction
- Hemiparesis on the side of the gaze deviation
- Doll’s eye maneuver and cold water caloric irrigation do not move the eyes to the opposite side
- Other signs of pontine dysfunction (lower motor neuron facial weakness, nystagmus, ataxia) will usually be present
-
Medullary lesion causing ocular lateropulsion
- Gaze deviation most pronounced under closed lids
- Have patients close their eyes; as they open them, you will see that the eyes were deviated toward the side of the lesion but move quickly back to straight-ahead gaze position; this phenomenon occurs most commonly in dorsolateral medullary infarction (See Dorsolateral Medullary (Wallenberg) Syndrome
-
Cerebral infarct/hemorrhage
- Depends on the underlying cause