Diplopia

- Seeing two copies of viewed objects
- Caused by optical disorders (“monocular diplopia”) or eye misalignment (“binocular diplopia”)
-
Monocular diplopia
- Patient reports seeing “ghost image"
- Ghost image persists when the unaffected eye is covered and disappears when the affected eye views the target through the pinhole
- If an uncorrected refractive error is the cause, the ghost image will disappear when the refractive error is corrected
- If a corneal or lens abnormality is the cause, it should be evident on slit lamp biomicroscopy; the ghost image should disappear on pinhole examination

-
Binocular diplopia
- Diplopia disappears when either eye is covered
- Caused by ocular misalignment
-
Trap: patients with ocular misalignment may not report diplopia if
-
They do not have adequate vision in one or both eyes
-
The image separation is very small, in which case they may report “blurred vision”
-
The image separation is very large, in which case they may be able to ignore the deviating image
-
The ocular misalignment began in early childhood, in which case they have suppressed the deviating image
-
They have diplopia but cannot communicate it
-
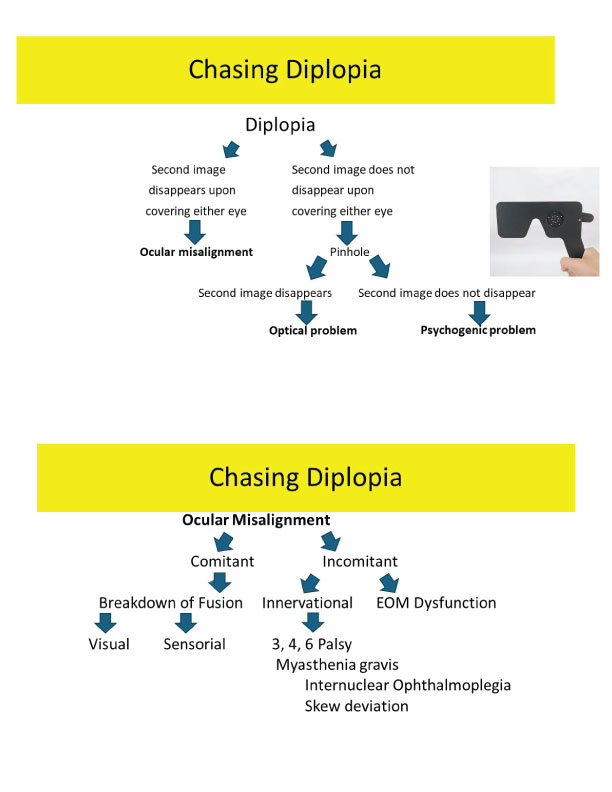
- Monocular diplopia of psychogenic origin, which does not disappear when the affected eye views the target through the pinhole
- Assess whether diplopia is monocular (optical disorder) or binocular (eye misalignment) by having the patient cover either eye and discovering if the diplopia persists (monocular diplopia) or disappears (binocular diplopia)
- Confirm that monocular diplopia is of optical origin by finding that the ghost image disappears when the affected eye views the target through the pinhole
-
Tip: if monocular diplopia does not disappear with the pinhole, it is likely of psychogenic origin
-
If you have confirmed that the diplopia is binocular, ask these questions
- Have you had other episodes of double vision in the past?”
- “Are the two images separated horizontally, vertically, or both?”
- “Does one of the images appear to be tilted?”
- “Is the double vision more apparent in any particular direction of your gaze?”
- “Since the double vision first appeared, do you believe that the separation of the images has increased, decreased, or stayed the same?”
- “Besides having double vision, do you have any other new symptoms?”
- Use the historical information to guide you in the assessment of eye movements (See Eye Movement Examination and eye alignment (See Eye Alignment Examination )
- If you have had limited experience in testing patients with diplopia, or if you are examining the patient at the bedside, perform the screening examination described in this video
- Optical causes of monocular diplopia can be inferred by results of the pinhole examination and confirmed with refraction and slit lamp examination
- Localization of the lesion responsible for binocular diplopia involves skillful assessment of eye movements and alignment
-
Trap: ocular misalignment causing diplopia may be present even when eye movements appear intact
- Diplopia may be relieved with
