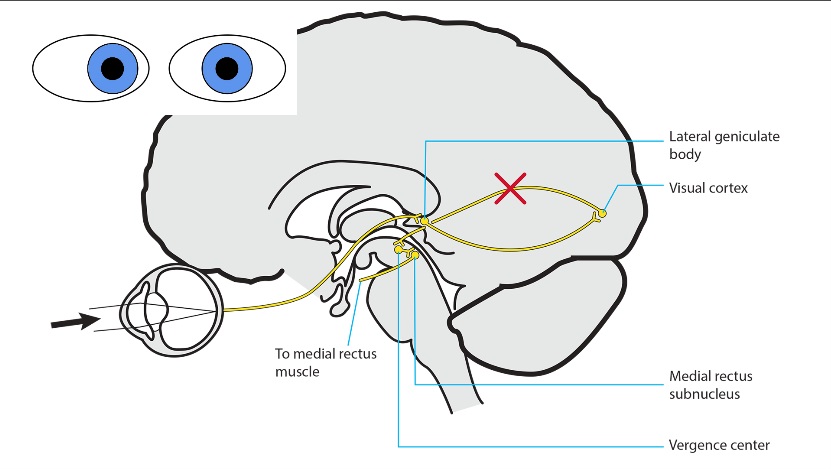
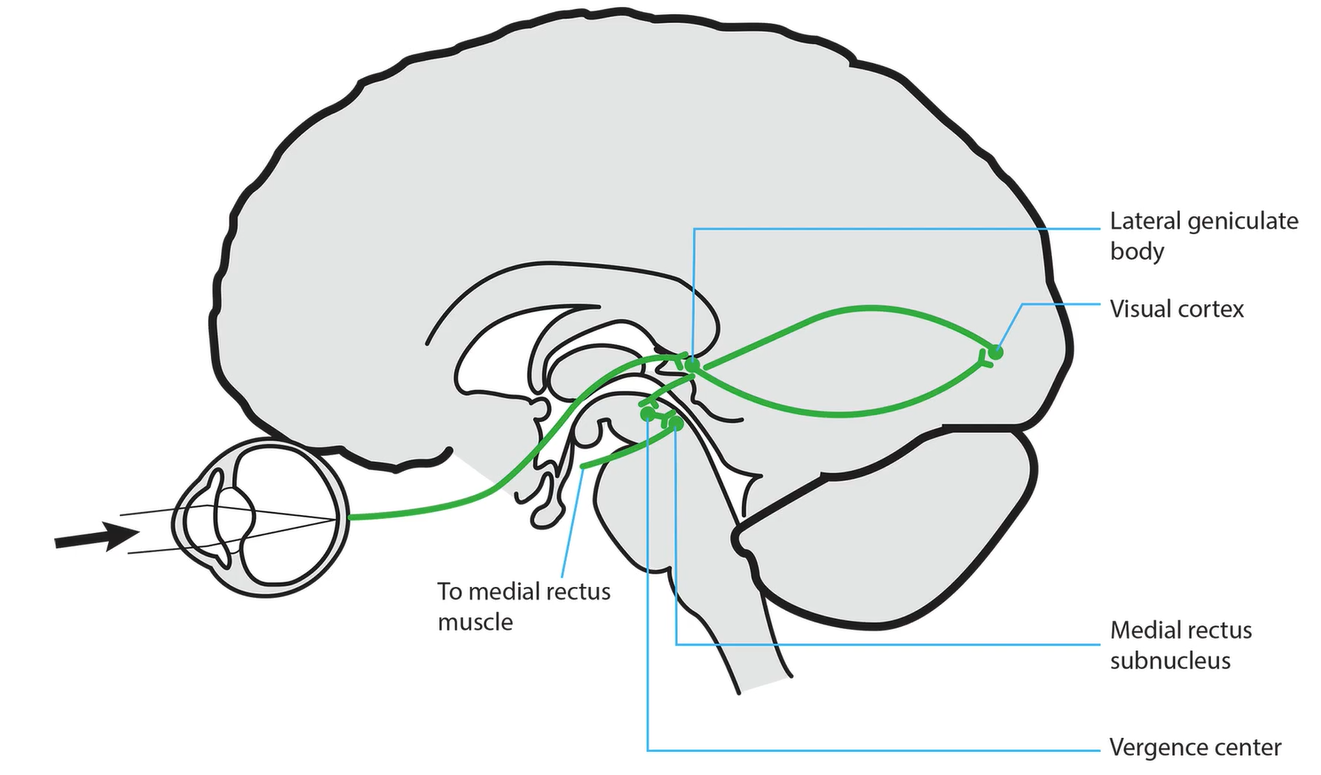
Vergence Pathway
-
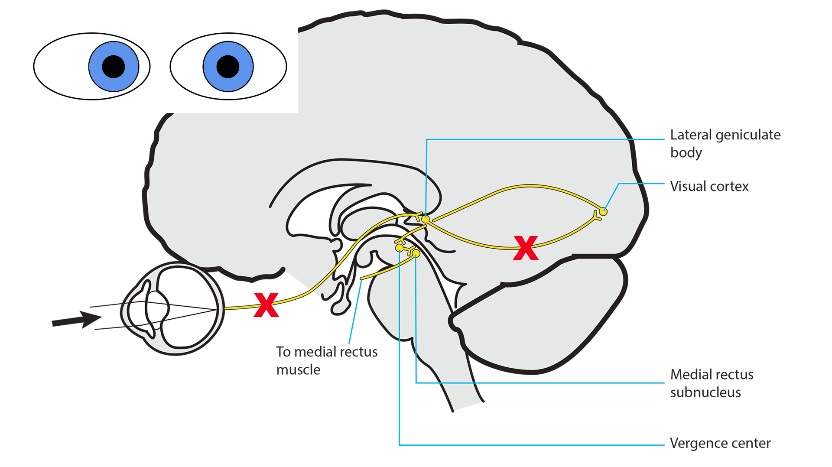
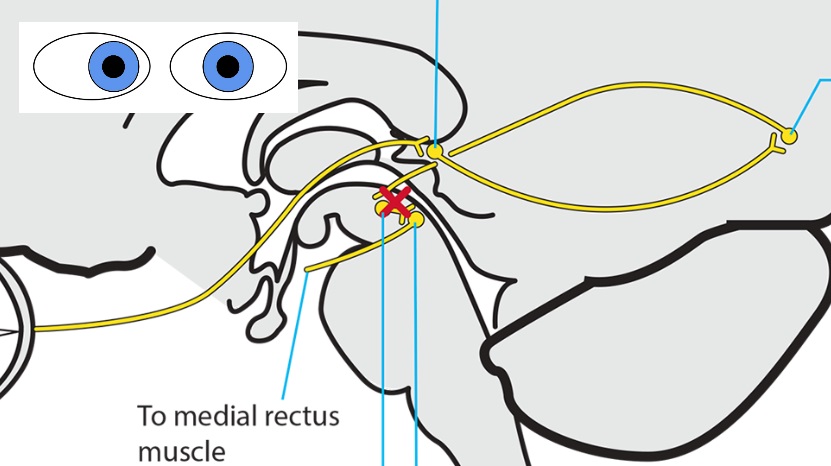
Lesion of the afferent visual pathway
- Produces reduced vision, which breaks fusion and causes comitant esotropia or exotropia (“sensory ocular misalignment”), but retains full amplitude of ocular ductions
- Common cause: any lesion of the visual pathway
-
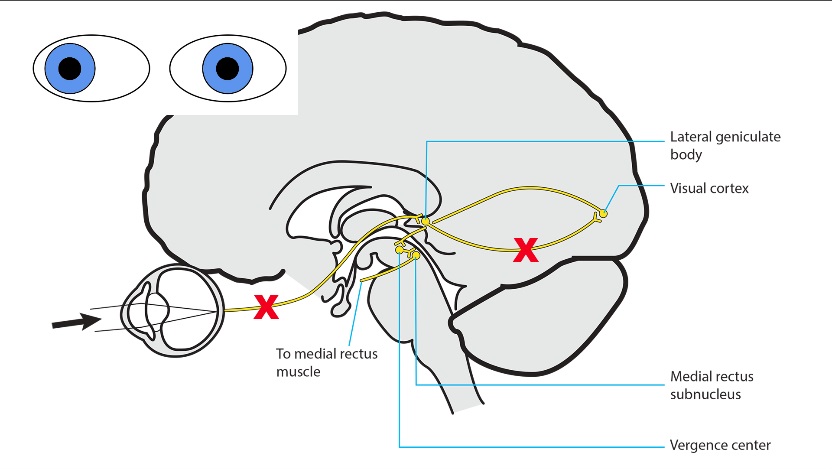
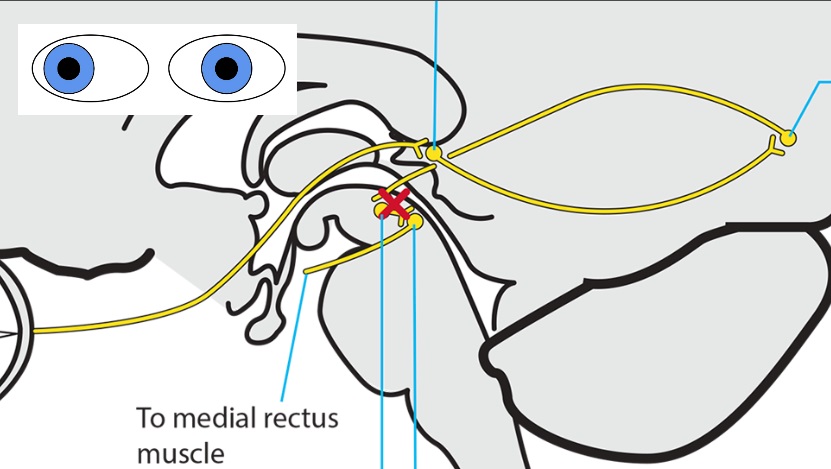
Lesion of the descending cerebral pathways from the occipital lobes on both sides
- Impairs transmission from the occipital lobes to the brainstem vergence center, which breaks fusion and causes comitant esotropia or exotropia, but retains full amplitude of ocular ductions
- Common causes: head trauma, encephalitis, narcotic or other neurotropic medication or drug use, sleep disturbance, fever, and increased intracranial pressure
-
Lesion of the thalamus or midbrain
- Disrupts the brainstem vergence center and causes comitant esotropia or exotropia, but retains full amplitude of ocular ductions
-
Tip: with a suspected thalamic or midbrain lesion, expect to find one or more of these clinical abnormalities
-
Impaired vertical gaze
-
Skew deviation
-
Lid retraction
-
Impaired pupil constriction to light with or without light-near dissociation (tectal pupils)
-
Third nerve palsy
-
Fourth nerve palsy
-