( of )
Correct: 0
Incorrect: 0
A 65 year old woman reports new double vision. She has been treated for diabetes, but says that her blood sugar has been normal and past ophthalmologic examinations have not disclosed retinopathy.
Where is the lesion?
Incorrect
Incorrect
Incorrect
Correct!
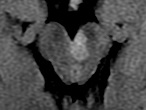 This patient has a left third nerve palsy, but it is not isolated! She also has a mild spastic right hemiparesis. (You might have thought that the left extremities were
showing reduced deep tendon reflexes, but actually it is the right extremity reflexes that are accentuated!) The combination of these features localizes to the cerebral
peduncle on the left side of the ventral midbrain. It is called a “Weber syndrome.” The peduncular lesion damages the descending corticospinal axons, which later cross to
the opposite side, causing a contralateral spastic hemiparesis that variably affects face, arm, and leg. Brain vascular imaging, which is urgent and mandatory in acute
isolated third nerve palsy to rule out aneurysm, is not the right approach here. You want high-definition MRI, which will visualize the midbrain. The most common cause is
an acute ischemic stroke, so you would be looking especially at a diffusion-weighted sequence.
This patient has a left third nerve palsy, but it is not isolated! She also has a mild spastic right hemiparesis. (You might have thought that the left extremities were
showing reduced deep tendon reflexes, but actually it is the right extremity reflexes that are accentuated!) The combination of these features localizes to the cerebral
peduncle on the left side of the ventral midbrain. It is called a “Weber syndrome.” The peduncular lesion damages the descending corticospinal axons, which later cross to
the opposite side, causing a contralateral spastic hemiparesis that variably affects face, arm, and leg. Brain vascular imaging, which is urgent and mandatory in acute
isolated third nerve palsy to rule out aneurysm, is not the right approach here. You want high-definition MRI, which will visualize the midbrain. The most common cause is
an acute ischemic stroke, so you would be looking especially at a diffusion-weighted sequence.
By the way, ischemic brainstem strokes often cover a small territory and will not be evident even on the best imaging. If it is negative, be sure you have excluded multifocal disease,
as might be seen in multiple sclerosis. Once that has been done, you can usually presume “imaging-occult” non-embolic ischemic brainstem stroke, and direct treatment at arteriosclerotic
risk factors.