( of )
Correct: 0
Incorrect: 0
A 65 year old man reports that two days ago he developed sudden severe pain around his right brow. One day later, he noticed that the right upper lid suddenly drooped. When he lifted the lid, he had double vision. He has been healthy except for controlled systemic hypertension. His ophthalmologic and neurologic examinations are normal except for what you see in this video.
What should you do?
Incorrect
Correct!
 You are looking at complete right upper lid ptosis together with impaired adduction, supraduction, and infraduction of the right eye. The pupils appear to be equal in size.
The rest of the ophthalmologic and neurologic examinations is normal, so this is probably an isolated pupil-sparing right third nerve palsy. In this age group, the overwhelmingly
likely cause is ischemia to the extra-axial (subarachnoid) portion of the nerve. Risk factors are those for arteriosclerosis. But a compressive lesion—most importantly an unruptured but
expanding intracranial aneurysm—could also rarely cause these abnormalities. Yes, it is true that aneurysmal compression of the third nerve usually causes mydriasis and impaired pupil
constriction, especially when the ocular ductions are so impaired. But that rule is disobeyed often enough to make it an imperfect guide. And consider this: if the aneurysm ruptures,
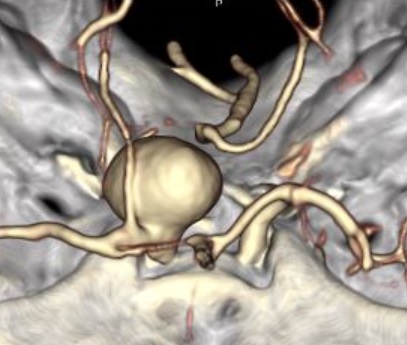
which could happen within hours to days, it could cause death. Therefore, you must immediately order a brain study that visualizes the basal arteries, looking especially at the
junction of the internal carotid and posterior communicating arteries, and at the junction of the basilar and superior cerebellar arteries. CT and MR angiography both have at least
a 95% chance of excluding aneurysms that compress the third nerve, but CT is more widely available, faster, and less subject to motion artefact than MRI. Its major disadvantage
is exposure to ionizing radiation, which should be avoided in children and pregnant women. A second disadvantage, relative to MRI, is poor visualization of brain parenchyma. So
CT would deny you the opportunity to visualize inflammation, small tumors, and recent or small infarction. Keep in mind that interpretation of vascular imaging requires expertise.
Aneurysms create subtle abnormalities that are often overlooked, even by well-trained radiologists! So, do not dismiss aneurysm unless the study adequately visualizes the key
areas and an expert has reviewed it. If the study is equivocal, or the features seem to exclude an ischemic cause (youth, minimal arteriosclerotic profile, partial somatic palsy
with some pupil involvement) you may have to ask a neuroradiologist to review it. If some equivocation about the study remains, consider ordering a brain MRI and MRA and even
a digital angiogram. On the other hand, if the imaging study is CERTIFIABLY negative, and the patient has an arteriosclerotic risk profile, you can fall back on a diagnosis of
presumed extra-axial ischemia and wait for resolution. In children, ischemia is such a rare cause that MRI and even lumbar puncture may be advised. Just to be clear: these
considerations apply only to “isolated third nerve palsy.” When there are other neuro-ophthalmic abnormalities, a giant work-up is always in store!
You are looking at complete right upper lid ptosis together with impaired adduction, supraduction, and infraduction of the right eye. The pupils appear to be equal in size.
The rest of the ophthalmologic and neurologic examinations is normal, so this is probably an isolated pupil-sparing right third nerve palsy. In this age group, the overwhelmingly
likely cause is ischemia to the extra-axial (subarachnoid) portion of the nerve. Risk factors are those for arteriosclerosis. But a compressive lesion—most importantly an unruptured but
expanding intracranial aneurysm—could also rarely cause these abnormalities. Yes, it is true that aneurysmal compression of the third nerve usually causes mydriasis and impaired pupil
constriction, especially when the ocular ductions are so impaired. But that rule is disobeyed often enough to make it an imperfect guide. And consider this: if the aneurysm ruptures,
which could happen within hours to days, it could cause death. Therefore, you must immediately order a brain study that visualizes the basal arteries, looking especially at the
junction of the internal carotid and posterior communicating arteries, and at the junction of the basilar and superior cerebellar arteries. CT and MR angiography both have at least
a 95% chance of excluding aneurysms that compress the third nerve, but CT is more widely available, faster, and less subject to motion artefact than MRI. Its major disadvantage
is exposure to ionizing radiation, which should be avoided in children and pregnant women. A second disadvantage, relative to MRI, is poor visualization of brain parenchyma. So
CT would deny you the opportunity to visualize inflammation, small tumors, and recent or small infarction. Keep in mind that interpretation of vascular imaging requires expertise.
Aneurysms create subtle abnormalities that are often overlooked, even by well-trained radiologists! So, do not dismiss aneurysm unless the study adequately visualizes the key
areas and an expert has reviewed it. If the study is equivocal, or the features seem to exclude an ischemic cause (youth, minimal arteriosclerotic profile, partial somatic palsy
with some pupil involvement) you may have to ask a neuroradiologist to review it. If some equivocation about the study remains, consider ordering a brain MRI and MRA and even
a digital angiogram. On the other hand, if the imaging study is CERTIFIABLY negative, and the patient has an arteriosclerotic risk profile, you can fall back on a diagnosis of
presumed extra-axial ischemia and wait for resolution. In children, ischemia is such a rare cause that MRI and even lumbar puncture may be advised. Just to be clear: these
considerations apply only to “isolated third nerve palsy.” When there are other neuro-ophthalmic abnormalities, a giant work-up is always in store!
Incorrect