( of )
Correct: 0
Incorrect: 0
A 57 year old man reports episodes of vertical diplopia that have become much more frequent within the past few months. Your examination shows a left hypertropia that increases on right gaze and disappears on left gaze. In right gaze, the hypertropia is greater in the upgaze position than in the downgaze position. The left hypertropia is also greater on left head tilt than on right head tilt. Double Maddox Rod testing shows 5 degrees of excyclodeviation.
Your favored diagnosis is
Correct!
 The pattern of ocular misalignment fulfills the features of the Parks-Bielschowsky “three-step test,” a strong indication of a fourth nerve palsy. The
main acquired causes of fourth nerve palsy-- trauma, tumor, ischemia, and inflammation--typically cause a hypertropia that is greater in downgaze than
in upgaze. Because the hypertropia in left gaze is greater here in upgaze than in downgaze, the palsy is likely to be ancient, possibly even congenital,
with “decompensation” in adulthood.
The pattern of ocular misalignment fulfills the features of the Parks-Bielschowsky “three-step test,” a strong indication of a fourth nerve palsy. The
main acquired causes of fourth nerve palsy-- trauma, tumor, ischemia, and inflammation--typically cause a hypertropia that is greater in downgaze than
in upgaze. Because the hypertropia in left gaze is greater here in upgaze than in downgaze, the palsy is likely to be ancient, possibly even congenital,
with “decompensation” in adulthood.
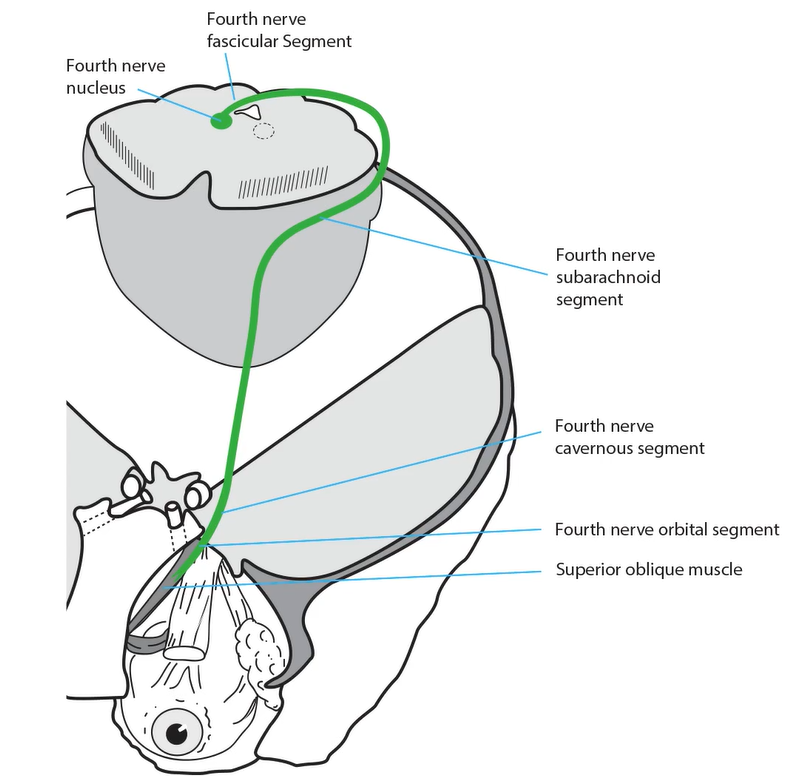
Why does this decompensation occur? Consider the anatomy of the superior oblique muscle and its tendon: it’s awkward. The muscle courses forward along the medial orbital wall, passes through a sleeve of dura called the trochlea, and turns more than 90 degrees to insert on the top of the eye.
Perhaps it does not take much for the muscle to fail if its innervation was not perfect to begin with.
The diplopia in this condition can sometimes be palliated with a spectacle prism. But because of the incomitance, the prism is usually an imperfect or temporary solution. Eye muscle surgery is the answer--a minor procedure such as weakening of the inferior oblique muscle.
With regard to the other answer choices here: although myasthenia gravis can produce any pattern of ocular misalignment, it is unlikely to cause such “three-step test” positivity. The same is true of inflammatory orbitopathy. Cerebral aneurysm can cause an isolated third nerve palsy, and you are right to worry about that diagnosis. However, the pattern of misalignment does not fit.
Intermittency of diplopia is likely to challenge you. Here are two good reasons for that phenomenon: 1) the misalignment is present only in certain fields of gaze, so that diplopia will occur only if the eyes move into those fields; 2) ocular fusion is breaking down because of age, fatigue, monovision, reduced vision in one eye, systemic illness, or CNS depressant medication, converting a phoria to a tropia. Notice how many actors can alter fusion!
Why does this decompensation occur? Consider the anatomy of the superior oblique muscle and its tendon: it’s awkward. The muscle courses forward along the medial orbital wall, passes through a sleeve of dura called the trochlea, and turns more than 90 degrees to insert on the top of the eye.
The diplopia in this condition can sometimes be palliated with a spectacle prism. But because of the incomitance, the prism is usually an imperfect or temporary solution. Eye muscle surgery is the answer--a minor procedure such as weakening of the inferior oblique muscle.
With regard to the other answer choices here: although myasthenia gravis can produce any pattern of ocular misalignment, it is unlikely to cause such “three-step test” positivity. The same is true of inflammatory orbitopathy. Cerebral aneurysm can cause an isolated third nerve palsy, and you are right to worry about that diagnosis. However, the pattern of misalignment does not fit.
Intermittency of diplopia is likely to challenge you. Here are two good reasons for that phenomenon: 1) the misalignment is present only in certain fields of gaze, so that diplopia will occur only if the eyes move into those fields; 2) ocular fusion is breaking down because of age, fatigue, monovision, reduced vision in one eye, systemic illness, or CNS depressant medication, converting a phoria to a tropia. Notice how many actors can alter fusion!
Incorrect
Incorrect
Incorrect