( of )
Correct: 0
Incorrect: 0
A 14 year old girl suffers head trauma in an automobile accident. When she recovers consciousness, she reports diplopia. Examination shows a right hypertropia in primary gaze position that increases on left gaze but converts to a left hypertropia on right gaze.
The responsible lesion is likely to be in the
Incorrect
Correct!
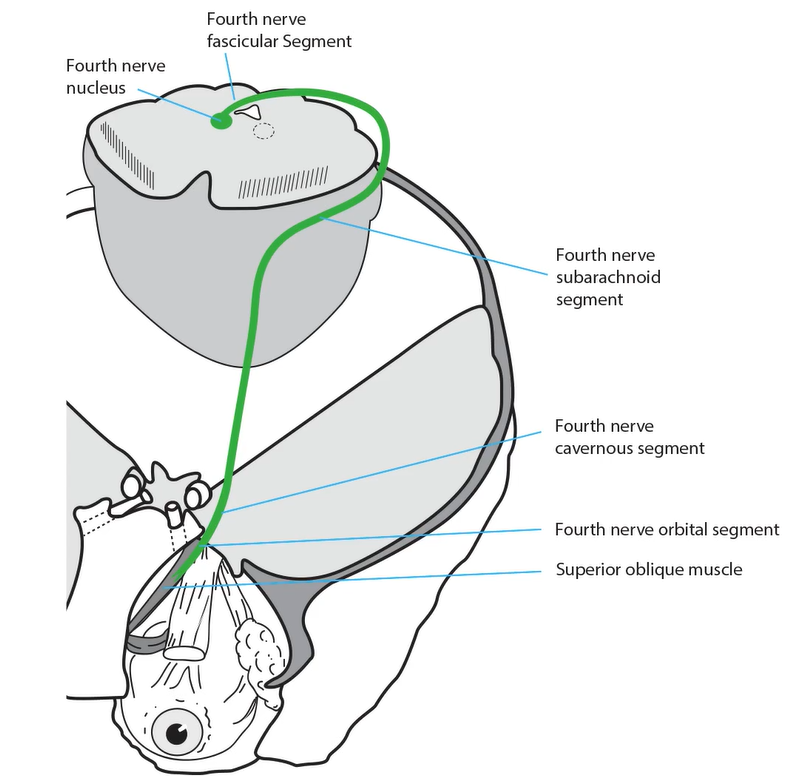
 When the right eye is higher in left gaze and the left eye is higher on right gaze, you are probably looking at BILATERAL fourth nerve palsies, especially in the setting of head trauma. In concussive head trauma, the brain moves more than its coverings, including the dura. As a result, the
dorsal midbrain slams into the rigid, knife-like inner margin of the tentorium cerebelli at exactly the place where the crossing fourth nerves exit from
the brainstem. The fourth nerves are often injured together, although usually asymmetrically.
When the right eye is higher in left gaze and the left eye is higher on right gaze, you are probably looking at BILATERAL fourth nerve palsies, especially in the setting of head trauma. In concussive head trauma, the brain moves more than its coverings, including the dura. As a result, the
dorsal midbrain slams into the rigid, knife-like inner margin of the tentorium cerebelli at exactly the place where the crossing fourth nerves exit from
the brainstem. The fourth nerves are often injured together, although usually asymmetrically.
Bilateral fourth nerve palsies create not only this pattern of hypertropia, but also a large (at least 10 degrees) excyclodeviation on Double Maddox Rod testing.
Many patients will also display an esotropia in downgaze. Do you know why?
In traumatic fourth nerve palsy, imaging generally does not show any pertinent abnormality, although sometimes there is hemorrhage in the caudal dorsal midbrain. If the concussive trauma also affects the more rostral dorsal midbrain, expect to see some features of a “dorsal midbrain syndrome,” especially reduced upgaze. With a high amount of excyclodeviation, patients may be symptomatic from torsional misalignment alone.
Recovery is delayed for months and is of variable degree. If recovery is minimal, eye muscle surgery may be necessary to align the eyes vertically and torsionally. It is challenging!
Bilateral fourth nerve palsies create not only this pattern of hypertropia, but also a large (at least 10 degrees) excyclodeviation on Double Maddox Rod testing.
Many patients will also display an esotropia in downgaze. Do you know why?
In traumatic fourth nerve palsy, imaging generally does not show any pertinent abnormality, although sometimes there is hemorrhage in the caudal dorsal midbrain. If the concussive trauma also affects the more rostral dorsal midbrain, expect to see some features of a “dorsal midbrain syndrome,” especially reduced upgaze. With a high amount of excyclodeviation, patients may be symptomatic from torsional misalignment alone.
Recovery is delayed for months and is of variable degree. If recovery is minimal, eye muscle surgery may be necessary to align the eyes vertically and torsionally. It is challenging!
Incorrect
Incorrect