( of )
Correct: 0
Incorrect: 0
A 66 year old man awakens from heart surgery with eyes deviated to the right. When you tell the patient to look to the left, neither eye moves beyond straight ahead gaze (“primary gaze position”) to the left. Yet when you move the patient’s head to the right, the eyes cross into left gaze. Vertical eye movements are intact and the eyes are aligned.

Where is the lesion?
Correct!
 In order to answer this question correctly, you had to know three things: 1) that horizontal saccades are generated in the cerebral hemispheres and that they move
the eyes toward the opposite side; 2) that the patient is displaying a dissociation between loss of volitional leftward horizontal saccades and preservation of the
leftward vestibulo-ocular reflex (“supranuclear ophthalmoplegia”); and 3) that the vestibulo-ocular reflex pathway is confined motorically to the brainstem.
In order to answer this question correctly, you had to know three things: 1) that horizontal saccades are generated in the cerebral hemispheres and that they move
the eyes toward the opposite side; 2) that the patient is displaying a dissociation between loss of volitional leftward horizontal saccades and preservation of the
leftward vestibulo-ocular reflex (“supranuclear ophthalmoplegia”); and 3) that the vestibulo-ocular reflex pathway is confined motorically to the brainstem.
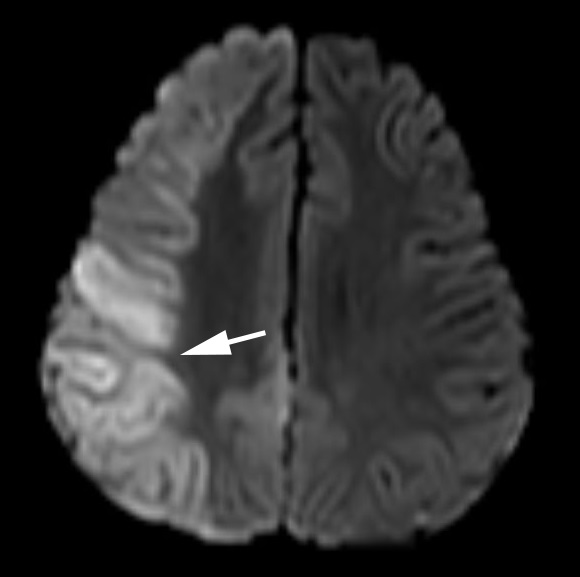
Acute right hemisphere lesions (usually infarcts or hemorrhages)--especially if they involve the parietal lobe or its efferent pathway--often produce ipsilateral gaze deviation and a supranuclear gaze disturbance, as described here. These phenomena are probably manifestations of “hemispatial neglect.” In fact, other aspects of hemispatial neglect are usually present, including extinction to double simultaneous stimulation in the visual, auditory, and tactile domains. The presence of multimodal--visual, auditory, and tactile--extinction favors neglect over a topographic disorder of vision such as a homonymous hemianopia. Patients with hemispatial neglect consistently ignore stimuli in one hemifield and bisect a line segment more toward the side of the lesion. When the lesion is severe, neglect will extend to lack of awareness of contralateral limbs (“anosognosia”). Fortunately, the manifestations of neglect gradually lessen with time, but may never completely disappear. This patient had a right parietal infarct.
Acute right hemisphere lesions (usually infarcts or hemorrhages)--especially if they involve the parietal lobe or its efferent pathway--often produce ipsilateral gaze deviation and a supranuclear gaze disturbance, as described here. These phenomena are probably manifestations of “hemispatial neglect.” In fact, other aspects of hemispatial neglect are usually present, including extinction to double simultaneous stimulation in the visual, auditory, and tactile domains. The presence of multimodal--visual, auditory, and tactile--extinction favors neglect over a topographic disorder of vision such as a homonymous hemianopia. Patients with hemispatial neglect consistently ignore stimuli in one hemifield and bisect a line segment more toward the side of the lesion. When the lesion is severe, neglect will extend to lack of awareness of contralateral limbs (“anosognosia”). Fortunately, the manifestations of neglect gradually lessen with time, but may never completely disappear. This patient had a right parietal infarct.
Incorrect
Incorrect
Incorrect