( of )
Correct: 0
Incorrect: 0
A 15 year old boy notices that when he looks upward, his eyes ache and that he gets double vision. You find that with attempted upward gaze, his eyes do not move upward, but instead they converge!
The responsible lesion lies in the
Correct!
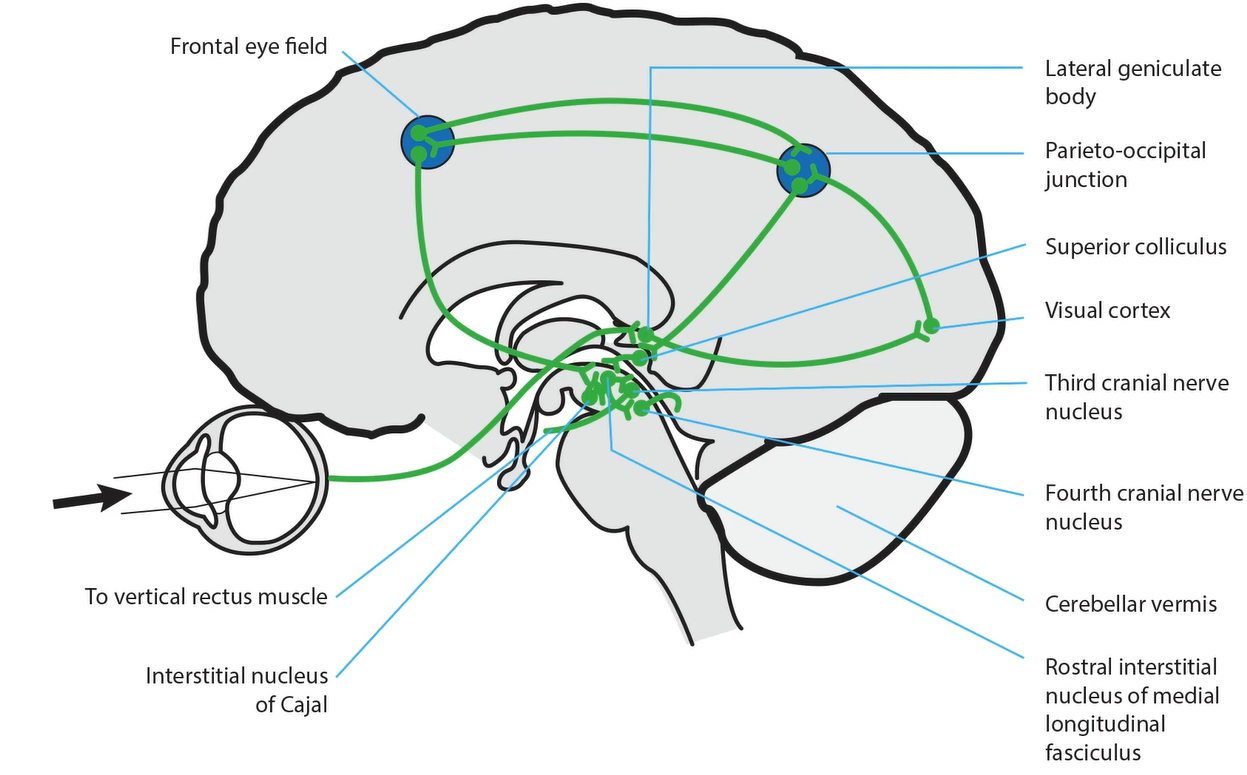
 This is an important neuro-ophthalmic landmark! Lying at the junction of the thalamus and midbrain, it mediates upward gaze by connecting the rostral interstitial nuclei of the medial
longitudinal fasciculus (RIMLF) and interstitial nucleus of Cajal (INC) on both sides.
This is an important neuro-ophthalmic landmark! Lying at the junction of the thalamus and midbrain, it mediates upward gaze by connecting the rostral
interstitial nuclei of the medial longitudinal fasciculus (RIMLF) and interstitial nucleus of Cajal (INC) on both sides. (Video: cartoon Upgaze) A
lesion here SELECTIVELY interferes with upward gaze, sparing downward gaze, which is mediated more ventrally.
This is an important neuro-ophthalmic landmark! Lying at the junction of the thalamus and midbrain, it mediates upward gaze by connecting the rostral interstitial nuclei of the medial
longitudinal fasciculus (RIMLF) and interstitial nucleus of Cajal (INC) on both sides.
This is an important neuro-ophthalmic landmark! Lying at the junction of the thalamus and midbrain, it mediates upward gaze by connecting the rostral
interstitial nuclei of the medial longitudinal fasciculus (RIMLF) and interstitial nucleus of Cajal (INC) on both sides. (Video: cartoon Upgaze) A
lesion here SELECTIVELY interferes with upward gaze, sparing downward gaze, which is mediated more ventrally.
When the posterior commissure is damaged by an intrinsic lesion of the caudal thalamus or pretectal or tectal midbrain regions, or by an extrinsic lesion like a pinealoma, expect elements of a “dorsal midbrain syndrome” (also called “pretectal syndrome,” “Sylvian aqueduct syndrome,” or “Parinaud syndrome” if you are French, “Koerber-Salus-Elschnig syndrome” if you are German). The clinical features of this syndrome include convergence retraction of the eyes on attempted upgaze, lid retraction (“Collier’s sign”), dilated pupils with light-near dissociation, and sometimes esotropia, exotropia, or skew deviation.
Why does a lesion here cause such diverse clinical phenomena? Disruption of upgaze produces a “spill-over” activation of all extraocular muscles, pulling the eyes backwards into the orbit. Because the medial recti are the most powerful muscles, the eyes tend to converge. Dilated pupils with light-near dissociation (“tectal pupils”) are attributed to interruption of the pupillary light reflex pathway in the dorsal midbrain. Esotropia and exotropia result from disruption of the vergence pathway in that region, and skew deviation results from interruption of the vestibulo-ocular pathway as it reaches the midbrain. This patient had a pinealoma.
Early diagnosis favors a better outcome of treatment. But even with early diagnosis, some features of a dorsal midbrain syndrome—especially upgaze deficiency and convergence-retraction--often linger. Why is this fact important? Because if upgaze deficiency and convergence-retraction are detected long after treatment, they should not be taken as signs of tumor recurrence or of a complication of radiotherapy, even if not previously documented!
When the posterior commissure is damaged by an intrinsic lesion of the caudal thalamus or pretectal or tectal midbrain regions, or by an extrinsic lesion like a pinealoma, expect elements of a “dorsal midbrain syndrome” (also called “pretectal syndrome,” “Sylvian aqueduct syndrome,” or “Parinaud syndrome” if you are French, “Koerber-Salus-Elschnig syndrome” if you are German). The clinical features of this syndrome include convergence retraction of the eyes on attempted upgaze, lid retraction (“Collier’s sign”), dilated pupils with light-near dissociation, and sometimes esotropia, exotropia, or skew deviation.
Why does a lesion here cause such diverse clinical phenomena? Disruption of upgaze produces a “spill-over” activation of all extraocular muscles, pulling the eyes backwards into the orbit. Because the medial recti are the most powerful muscles, the eyes tend to converge. Dilated pupils with light-near dissociation (“tectal pupils”) are attributed to interruption of the pupillary light reflex pathway in the dorsal midbrain. Esotropia and exotropia result from disruption of the vergence pathway in that region, and skew deviation results from interruption of the vestibulo-ocular pathway as it reaches the midbrain. This patient had a pinealoma.
Early diagnosis favors a better outcome of treatment. But even with early diagnosis, some features of a dorsal midbrain syndrome—especially upgaze deficiency and convergence-retraction--often linger. Why is this fact important? Because if upgaze deficiency and convergence-retraction are detected long after treatment, they should not be taken as signs of tumor recurrence or of a complication of radiotherapy, even if not previously documented!
Incorrect
Incorrect